
ACL
What is the ACL?
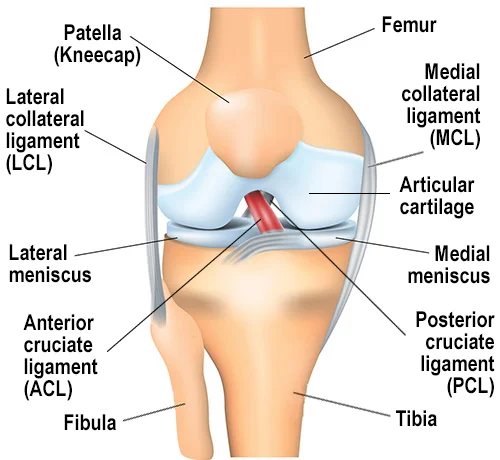
The Anterior Cruciate Ligament (ACL) connects the femur (thigh bone) to the tibia (shin bone) and plays a critical role in knee stability during rotational movements, pivoting and jumping.
How is the ACL injured?
Typical causes include sudden stops, changes of direction, improper landings from jumps, and direct contact injuries. Sports such as basketball, soccer, football and skiing report high rates.
Signs & Symptoms
- “Pop” sound at the time of injury
- Rapid swelling within hours
- Inability to continue activity or bearing full weight
- Feeling of knee “giving way” or instability during pivoting
Diagnosis & Pre-Op Evaluation
Diagnosis typically involves clinical tests (e.g., Anterior drawer test, Lachman’s test, pivot shift) and MRI scanning to assess ligament tear, meniscus/cartilage damage or bone alignment.
At our hospital, we use advanced imaging + planning protocols to choose the right graft and strategy for your individual needs.
Treatment Options
Non-Surgical Management
For partial tears, low-demand activity levels or when no instability exists, a combination of rehabilitation, bracing and activity modification may suffice.
Surgical Reconstruction
Complete ACL tears or persistent instability in active patients typically benefit most from arthroscopic ACL reconstruction. At our centre, this means:
- Keyhole (arthroscopic) surgery → smaller scars & faster recovery
- Personalised graft choice (Hamstring / BTB / Quadriceps / Allograft)
- Precision tunnel placement & fixation with modern implants
- Surgeon-led physiotherapy from day one
Recovery Timeline
- Day 0–1: Weight-bearing with aid, pain and swelling control
- Week 2–4: Full extension, flexion up to ~120°, early quad/hamstring work
- Week 6–12: Strength, balance training; light jogging may begin once cleared
- Month 4–6+: Sport-specific drills and full return to pivoting sports (clearance-based)
FAQ

Is arthroscopic ACL better than open surgery?
Yes, keyhole (arthroscopic) approaches generally allow reduced pain, earlier motion and faster recovery — though long-term stability depends on correct technique and rehabilitation.
Which ACL graft is the best?
- Bone–Patellar Tendon–Bone (BPTB) – Best choice for competitive athletes.
- Hamstring Tendon (Semitendinosus ± Gracilis) – Best for general population & non-contact sports.
- Quadriceps Tendon (± Bone Plug) – Excellent alternative to BPTB.
- Allograft (Cadaver Graft) – Avoid in young athletes
Do all ACL tears need surgery?
No. Partial tears or low-activity lifestyles may be managed without surgery. But persistent instability or pivoting sports favour surgical reconstruction.
When can I return to sport after ACL reconstruction?
Return to sport (RTS) after ACL reconstruction is based on function, not just time.
Returning before 6 months → 2–4× higher re-injury risk
Young athletes (<25 yrs) have highest re-tear risk
Rehab quality matters more than graft type
Minimum 9 months for pivot sports
What about meniscus injury along with ACL?
If your MRI shows a meniscus tear along with ACL injury, we prioritise meniscus repair or preservation to protect knee cartilage and longevity.